What an amazing RISE Summit on Social Determinants of Health it’s been! Day two delivered another impressive lineup of compelling speakers, timely discussions, and cross-sectional connection.
Our first session of the day featured an insightful spotlight on an innovative financing solution and upstream economic model that works with Len Nichols, Ph.D., non-resident fellow, Health Policy Center, Urban Institute. Throughout the presentation, Nichols shared an in-depth look at how to utilize a Collaborative Approach to Public Good Investments (CAPGI) as a sustainable financing tool for communities to improve health and wellbeing, create a stronger community, and lower costs, all while addressing the free rider problem.
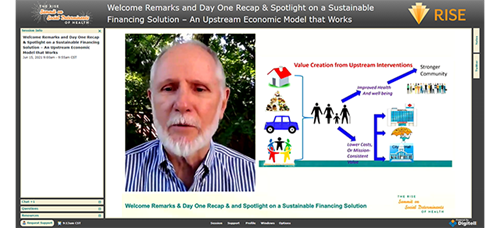
As a solution to the public good and free rider problem, Nichols and his colleagues developed the CAPGI model, which aims to make upstream SDoH investments sustainable by establishing a trusted and fair financing system. Following the CAPGI model, stakeholders will only communicate with a designated trusted broker regarding their “bid,” the amount they are willing pay toward the initiative. Based on the funds offered by each stakeholder, the trusted broker then assigns fair prices to each stakeholder so that any surplus beyond the total cost of the initiative is shared. All contributions and sustainability are based on enlightened self-interest, noted Nichols.
To make upstream SDoH investment sustainable, the model also includes two “fairness constraints,” explained Nichols:
- No one pays more than they bid, and everyone shares in the surplus.
- Each stakeholder shares the available surplus in equal proportion.
Since sharing the CAPGI model publicly, Nichols and his colleagues have heard from communities across the country wanting to implement the innovative solution. After conducting a serious application process, Nichols and team selected 10 of the most promising applicants to help implement the CAPGI model within their communities between 2020-2022.
“We realized we touched a nerve,” he said. “The truth is, there’s a hunger, a sense of urgency that we have to figure out as a country how to deal with upstream activities that have been underinvested in for so long.”
We then heard an insightful panel discussion on the intersection of sustainability and care delivery as industry thought leaders explored innovative funding mechanisms and payment models. Throughout the session, panelists evaluated creative funding mechanisms, their examples of funding models that work, and SDoH incentives to build into value-based agreements between health plans and health care providers. Among the panel’s many takeaways:
- Social determinants are slowly making their way into the U.S. health care landscape and payment models. It started with health care organizations screening members for SDoH and then referring patients/members for services. The next step is to gather the data on what happened after the referral was made, explained Melissa Sherry, vice president of social care integration at Unite Us, where she designs payment technology services to increase funding for social care and community capacity building. “There has to be a closed loop beyond screening and referring to help community partners and find out whether they have the capacity to accept the referral. The next step is paying them,” she said.
- Some pilot programs are making headway in this area, she said. For example, the Healthy Opportunities Pilots in North Carolina will cover the cost of approved services related to housing, food, transportation, interpersonal safety, and toxic stress that directly impact people’s health outcomes and health care costs. And in California managed care plans are exploring how to pay for community-based services that can replace an expensive health care service. If successful, these programs might lead to policy change and opportunities for health plans to start this funding, Sherry said.
- The work takes a lot of time, flexibility, and can’t be rushed, said Robert Gibson, chief strategy and innovation officer at Volunteers of America. You need to give the local community the power and time to involve the right community partners to build a health equity approach, he said. “It takes a lot longer than you expect going into the partnership, and it takes longer at every stage of the work…relationship building, trust building, creative financing, structuring, contracting, takes about five times longer than initially expected. Showing the payoff of an actual intervention takes longer,” he said. And the kinks must be worked out on the ground while the organizations deliver the service and then they can collaborate with managed care organizations or the hospital system to align outcomes.
- There is no ideal funding formula but there are options organizations can consider, according to Stuart Butler, senior fellow in economic studies at The Brookings Institution. Those options include working closely with state and county officials to push for a special body to coordinate funding. If that body is put in place, it will allow individual budget managers the cover they need to go outside their comfort zone and help other organization. Another mechanism is to identify or create a pool of special funds for collaboration in the nongovernment sector (such as wellness funds focused on initiatives to improve the health of children). Other possible opportunities are via funding available under the American Rescue Plan and previous stimulus bill packages. “If you look around your community, you will find a lot of opportunity,” he said. “If we enforce that with better policies and regulations from the federal government and state to make it easier for these partnerships to get together, it will really take off.”
- COVID-19 has forced health care organizations to think differently about the role of community-based organizations. For example, vaccination efforts have led health care organizations to now realize the benefit of working with local organizations and churches. “I’m reasonably optimistic that health systems will wise up that there is value in collaboration and cooperating with community organizations,” said Alexander Plum, director of clinical and social health integration at Henry Ford Health System.
Throughout the afternoon, attendees split into concurrent track sessions, which included a spotlight on Virtua Health’s innovative mobile grocery store program, a look at how to improve results by measuring consumer behavior and SDoH, a fireside chat on the technologies and strategies behind Highmark Health’s closed loop SDoH programs, and crossing the digital divide in government programs.
The last session of the conference showcased panel perspectives on SDoH innovation and what’s on the horizon, including examples of innovative best practices, program examples, and perspectives on the current and future state of SDoH in the managed care space. A key focus for the panel was the ongoing journey in data collection in the SDoH space as well as showing ROI in SDoH initiatives. While panelists shared their efforts to collect individual insights through methods such as screening assessments and ICD-10 code utilizations, they all recommended supplementing data with any publicly available data, such as the CDC Social Vulnerability Index and the National Equity Atlas.
When it comes to ROI in SDoH efforts, the panelists emphasized the need for a shift in mindset that while some outcomes will be financial ones, others are going to be health outcomes. “It’s not always a financial return,” said Eve Gelb, senior vice president, member and community health, SCAN Health Plan. “We use the term VOI instead of ROI, the value on investment.”
Looking ahead, the panel is excited to continue the momentum gained in the SDoH space. "I'm thrilled how the SDoH silo is picking up steam, and I'm hopeful we're beyond a place where it stops," said Deb Donovan, vice president, SDOH strategy & operations, Highmark. "I just see great opportunities in front of us that we're moving to improving health and not just health care."
In her closing remarks, Conference Chairperson and RISE SDoH Community Chair Ellen Fink-Samnick left us with a few words of encouragement. “There is so much great work happening, so much great work that has happened, and we are seeing the results. We’re seeing the outcomes in all sorts of ROI, from human, clinical, and fiscal outcomes. Know that your efforts are working.”